Should You Give the First Dose of Antibiotics IV Before Discharging Home on Oral Antibiotics?
Bottom Line Up Top: In patients with infectious processes that are stable for discharge home, there is no role for giving a first dose of antibiotics IV in the ED.
Clinical Scenario: A 45-year-old woman with hypertension presents with a productive cough and fever. Her vitals are: HR 115, BP 120/80, Temp 102.8, O2 Sat 99% on RA, RR 18. A CXR demonstrates a right middle lobe opacity. After acetaminophen, her HR is 82 and her temp is 98.5. You decide she is stable to be discharged home on levofloxacin (See REBEL EM for antibiotic coverage in CAP) but consider giving her a first dose intravenously.
What Your Gut Says: Give the first dose IV! Jump start those antibiotics so the patient will get better faster.
What The Evidence Says:
Many medical professionals believe that IV antibiotics are superior to oral antibiotics. This feels intuitive as the IV route seems like it would be stronger, faster, and fix the patient better than the oral route. Except for patients with poor gut absorption or those with critical infectious processes such as septic shock or necrotizing fasciitis, this belief appears to be unfounded. The majority of antibiotics we prescribe on a regular basis have excellent bioavailability through the oral route (see table below) (MacGregor 1997). For example, the bioavailability for oral levofloxacin, as used in our patient, is 99%. The infection doesn’t care how the antibiotic reached it, only that it did in fact get there.


While the effectiveness of antibiotics can be influenced by host factors or the dose given (i.e. a low bioavailability can be overcome by giving a larger dose), bioavailability is still a good place to start. Even better would be to see studies comparing one route to the other. We have a number of studies in adults and kids that do just that: Links to each study are in the Caption Below

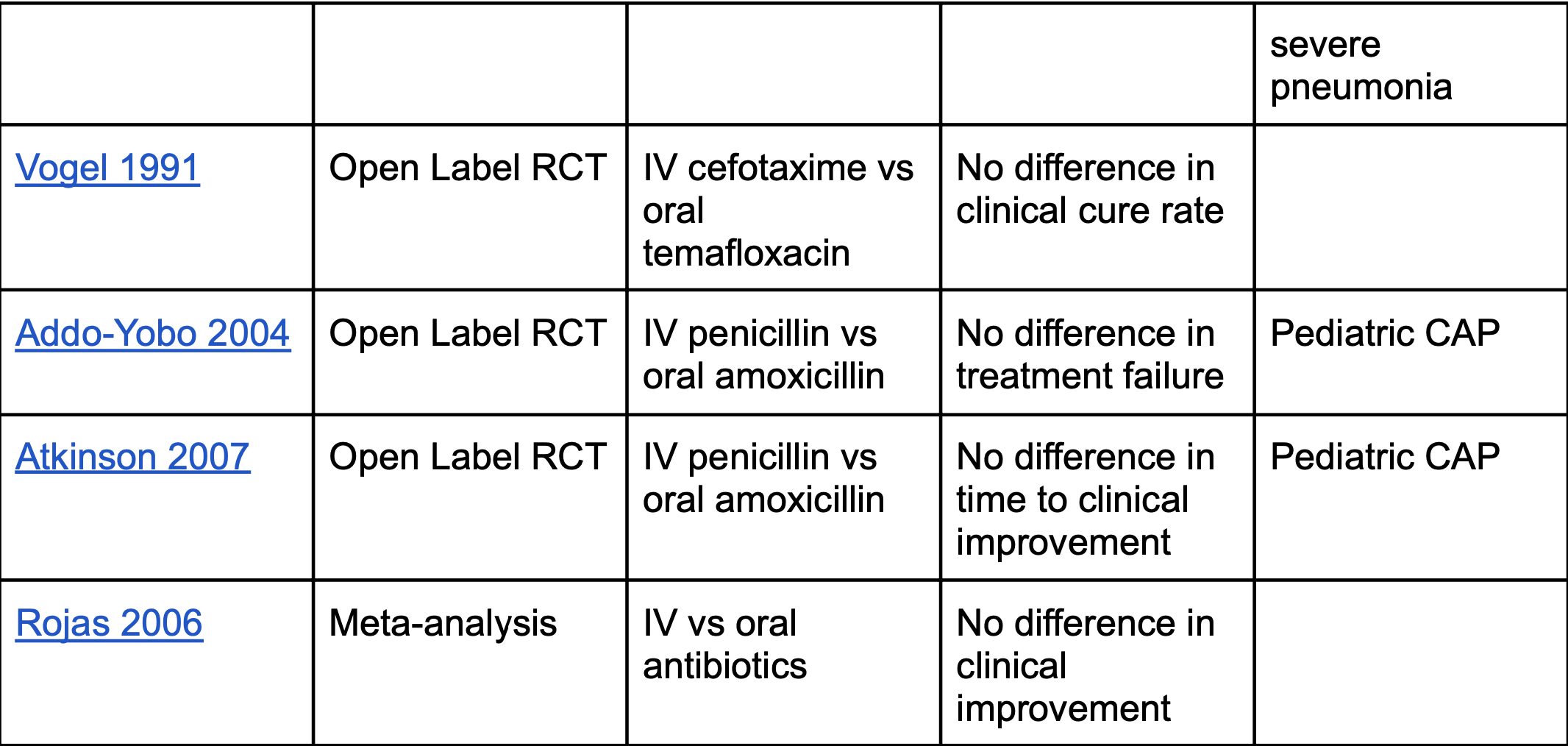
While none of these studies is perfect, (we have no large, multicenter, randomized, controlled, double-blind studies) there isn’t a single study showing either superiority of IV antibiotics or inferiority of oral antibiotics. This finding persists when looking at a number of other infections including skin and soft tissue infections (SSTI) (First10EM), pyelonephritis (Strohmeier 2014) and even bone and joint infections (Li 2019). Additionally, multiple studies demonstrate increased harm with IV antibiotics such as increased rate of diarrhea (Haran 2014), complications from IV placement (Li 2015), and increased length of stay or cost (Lorgelly 2010).
Bottom Line: The weight of the evidence shows no benefit in treating a stable patient with CAP, SSTI or UTI with IV antibiotics or with a single dose of IV antibiotics followed by an oral antibiotic course. Furthermore, there are real harms associated with unnecessary IV antibiotics. The practice of a single dose of IV antibiotics prior to discharging home with a course of oral antibiotics should be ended.
Read More
First10EM: Magical Thinking in Modern Medicine: IV Antibiotics for Cellulitis
First10EM: Oral Antibiotics are Equivalent to IV (Again) - The OVIVA Trial
References
MacGregor RR, Graziani AL. Oral administration of antibiotics: a rational alternative to the parenteral route. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 1997; 24(3):457-67. PMID: 9114201
Siegel RE et al. A prospective randomized study of inpatient iv. antibiotics for community-acquired pneumonia. The optimal duration of therapy. Chest. 1996; 110(4):965-71. PMID: 8874253
Oosterheert JJ, Bonten MJ, Schneider MM. Effectiveness of early switch from intravenous to oral antibiotics in severe community acquired pneumonia: multicentre randomised trial. BMJ (Clinical research ed.). 2006; 333(7580):1193. PMID: 17090560
Castro-Guardiola A et al. Efficacy and safety of oral and early-switch therapy for community-acquired pneumonia: a randomized controlled trial. The American journal of medicine. 2001; 111(5):367-74. PMID: 11583639
Vogel F, Lode H. The use of oral temafloxacin compared with a parenteral cephalosporin in hospitalized patients with pneumonia. The Journal of antimicrobial chemotherapy. 1991; 28 Suppl C:81-6. PMID: 1664833
Addo-Yobo E, et al. Oral amoxicillin versus injectable penicillin for severe pneumonia in children aged 3 to 59 months: a randomised multicentre equivalency study. Lancet 2004; 364: 1141-8. PMID: 15451221
Atkinson M et al. Comparison of oral amoxicillin and intravenous benzyl penicillin for community acquired pneumonia in children (PIVOT trial): a multicentre pragmatic randomised controlled equivalence trial. Thorax 2007; 62(12): 1102-6. PMID: 17567657
Rae N et al. Oral versus intravenous clarithromycin in moderate to severe community-acquired pneumonia: an observational study. Pneumonia 2017. PMID: 28702304
Rojas MX, Granados C. Oral antibiotics versus parenteral antibiotics for severe pneumonia in children. Cochrane Database Syst Rev 2006(2). PMID: 16625618
Strohmeier Y et al. Antibiotics for acute pyelonephritis in children. The Cochrane database of systematic reviews. 2014; PMID: 25066627
Li HK et al. Oral versus Intravenous Antibiotics for Bone and Joint Infection. The New England journal of medicine. 2019; 380(5):425-436. PMID: 30699315
Haran JP, Hayward G, Skinner S. Factors influencing the development of antibiotic associated diarrhea in ED patients discharged home: risk of administering IV antibiotics. The American journal of emergency medicine. 2014; 32(10):1195-9. PMID: 25149599
Li HK, Agweyu A, English M, Bejon P. An unsupported preference for intravenous antibiotics. PLoS medicine. 2015; 12(5):e1001825. PMID: 25992781
Lorgelly PK et al. Oral versus i.v. antibiotics for community acquired pneumonia in children: a cost minimisation analysis. Eur Resp J 2010; 35: 858-64. PMID: 19717479