Case: 15-year-old female who was seen in the ED 5 days ago for a forearm fracture, but no other significant PMH, presenting with a syncopal episode. Patient was well until this morning, when mother was brushing her hair in the bathroom to get ready for her orthopedic follow-up appointment. At that time, the patient felt dizzy, her vision went black, and she passed out. The patient remembers waking up in the kitchen (to where she was carried by her father). She was immediately acting at baseline, with no confusion/drowsiness afterwards but feels tired. She denied significant pain from her forearm or other source prior to the episode of syncope.
Syncope
Definition: Syncope is an abrupt loss of consciousness due to an interruption of energy sources to the brain, usually because of a sudden reduction of cerebral perfusion.
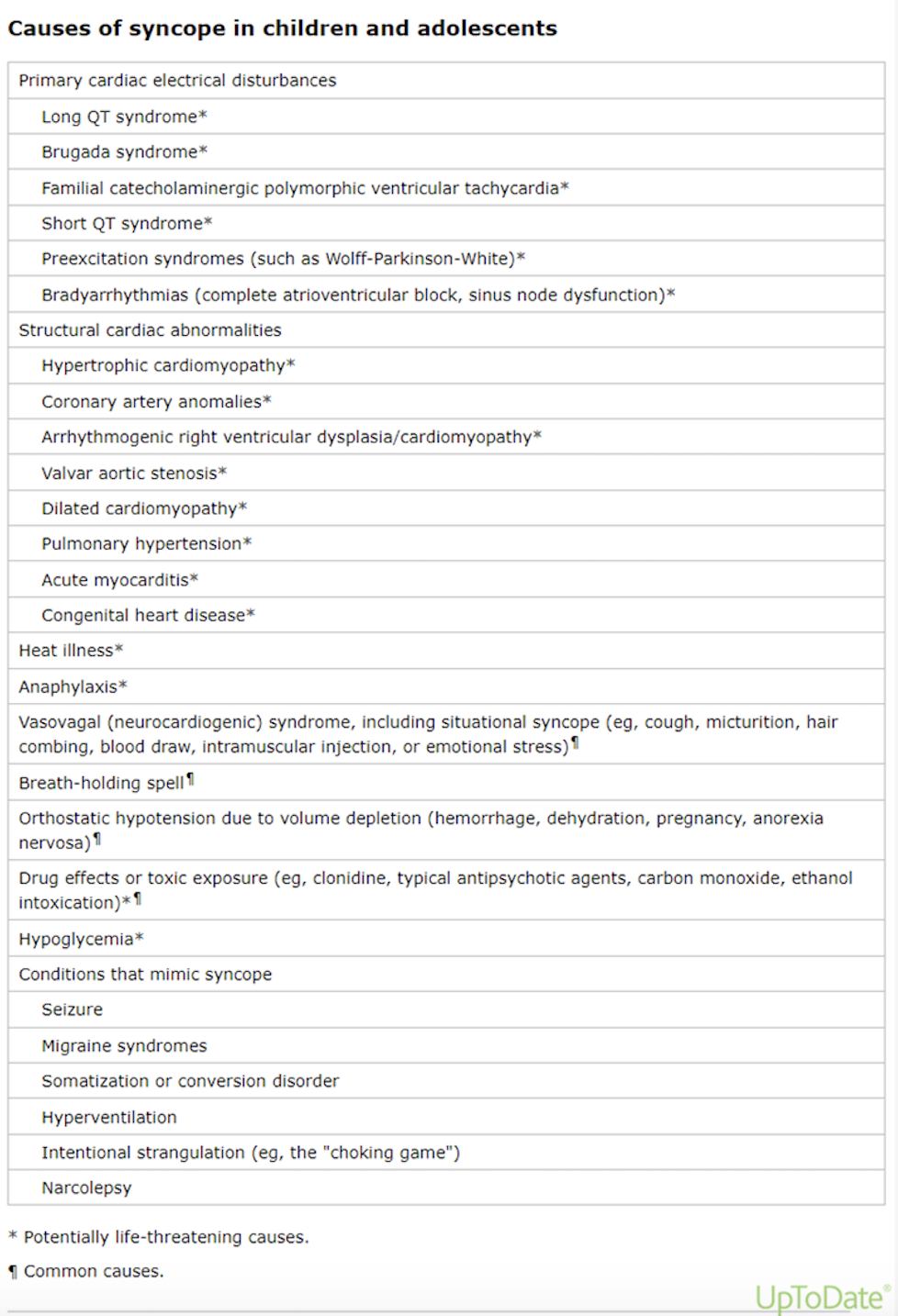
Etiology: Various causes from benign to life threatening. Think cardiac versus non-cardiac.
Cardiac – think of structural versus dysrhythmia.
Non-cardiac –
Neurocardiogenic/vasovagal is the most common.
Also consider neurologic causes - seizure, TIA
metabolic abnormalities
orthostatic hypotension
anemia (especially in menarchal patients)
hyperventilation (hypocapnia à respiratory alkalosis à cerebral vasoconstriction à decreased cerebral perfusion à syncope)
tox
psych (conversion disorder, pseudosyncope)
pulmonary embolism
trauma (commotio cordis)
And many more!
There’s also convulsive syncope – convulsive motor movements during cerebral hypoperfusion with syncope. Convulsive syncope is usually brief (<20 seconds), with usually no following confusion/drowsiness vs in seizure. So, it’s very important to get detailed history of events to help differentiate.
Evaluation: using history and physical to guide the work-up going through the differential diagnosis.
Important history questions – who (any witness), potential trigger, positional, symptoms/situation before (prodrome), during and after event (patient recollection of event?), stress (emotional), hydration status and last PO (hypoglycemia), cardiac questions, neurologic questions, recurrence, especially ask about family history of neurologic disorders and significant cardiac disease or sudden death – common in concerning cardiac conditions (see table below).
Findings concerning for cardiac cause include chest pain or palpitations prior to event, lack of prodrome, occurring with exertion.

Physical exam – assess for hydration and anemia, evaluate for cardiac causes (pathologic murmur), neuro causes.
Testing - Usually at least an EKG (minimally invasive and lots of information on life-threating conditions), maybe FS, maybe electrolytes, upreg, maybe CBC (especially in females if they have heavy menstrual periods).
Concerning EKG findings – Look for WPW, Prolonged QTc (QTc > 460ms), Shortened QTc – (QTc < 320ms), AV blocks, Brugada, HOCM, etc.
What is neurogenic/vasovagal syncope?
Autonomic activation leads to a hyperactive parasympathetic cardioinhibitory response and/or a diminished sympathetic response leading to vasodepression (bradycardia and hypotension) and syncope. It is the cause of more than 50% of the visit for syncope to the ED.
Triggers:
Triggers include standing or stress (physical/orthostatic or emotional), pain, and reflux triggers such as swallowing, coughing, yawning, hair grooming, urination and, post-tussive.

Presentation:
Patient had a classic prodrome which includes lightheadedness, feeling warm or cold, sweating, palpitations, nausea or abdominal discomfort, blurry or tunnel vision, decreased hearing or a "whooshing" sound in the ears, pallor noted during the episode, and fatigue after recovery.
Patients can have vasovagal syncope in the sitting or standing position. During an episode, people often try to sit the patient upright, which causes the patient to syncopize repeatedly as they have not generated enough blood pressure to push blood against gravity up to the head. This is why we recommend the patient be laid flat with the legs lifted to allow for blood flow to the head.
Treatment: Supportive – encourage increased salt and water intake, regular meals, avoidance of triggers.