Hope everyone had a great holiday weekend. Here is this week's US education for the week. Another save by POCUS in my eyes.
11 yo F presents with 4 days of unilateral left temporal swelling. Denies any direct trauma. No change in vision. No fevers or chills. Denies any redness to the skin. Never had this before. No pain. No other complaints.
T 98.2 F HR 88 BP 104/59 RR 18 o2 100% RA
PE well appearing, NAD, comfortable appearing
HEENT + fluctuant edematous well circumscribed lesion to left temporal region no overlying erythema nontender to touch no orbital ecchymosis EOMI clear conjunctiva bilaterally
nares patent pharynx clear no dental abscess or tenderness to palpation
CVS s1 s2 no murmurs
Lungs cta bilaterally
Abs soft ntnd no hsm
ext from x 4
Skin no rashes wwp
POCUS performed because... well duhh....
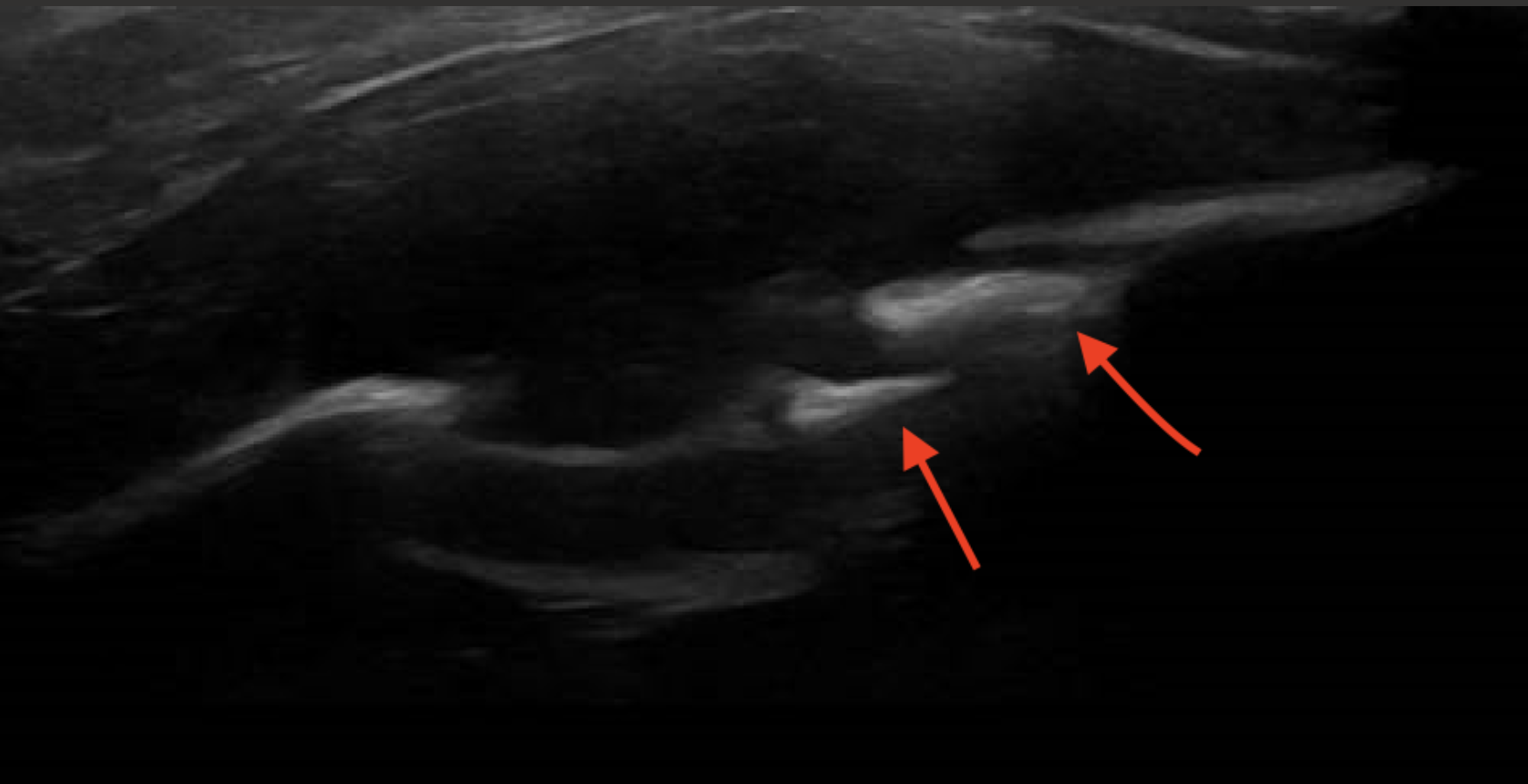
You scanned the area of clinical concern, along the left temporal region, in both transverse and sagittal views with your linear probe. You start looking at the soft tissue in the area then notice the skull which is the hyperechoic bone posterior to the lesion.
Upon review of the images, you identify no surrounding cellulitis or "cobblestoning". No loss of soft tissue architecture making this less likely inflammatory/infectious in nature. There is a hypoechoic soft tissue lesion(circle in red). The hyperechoic speckles (red arrows) are showing discontinuity in the cortex of the bone signifying bony erosion of this lesion.
A cine clip is here to show better image
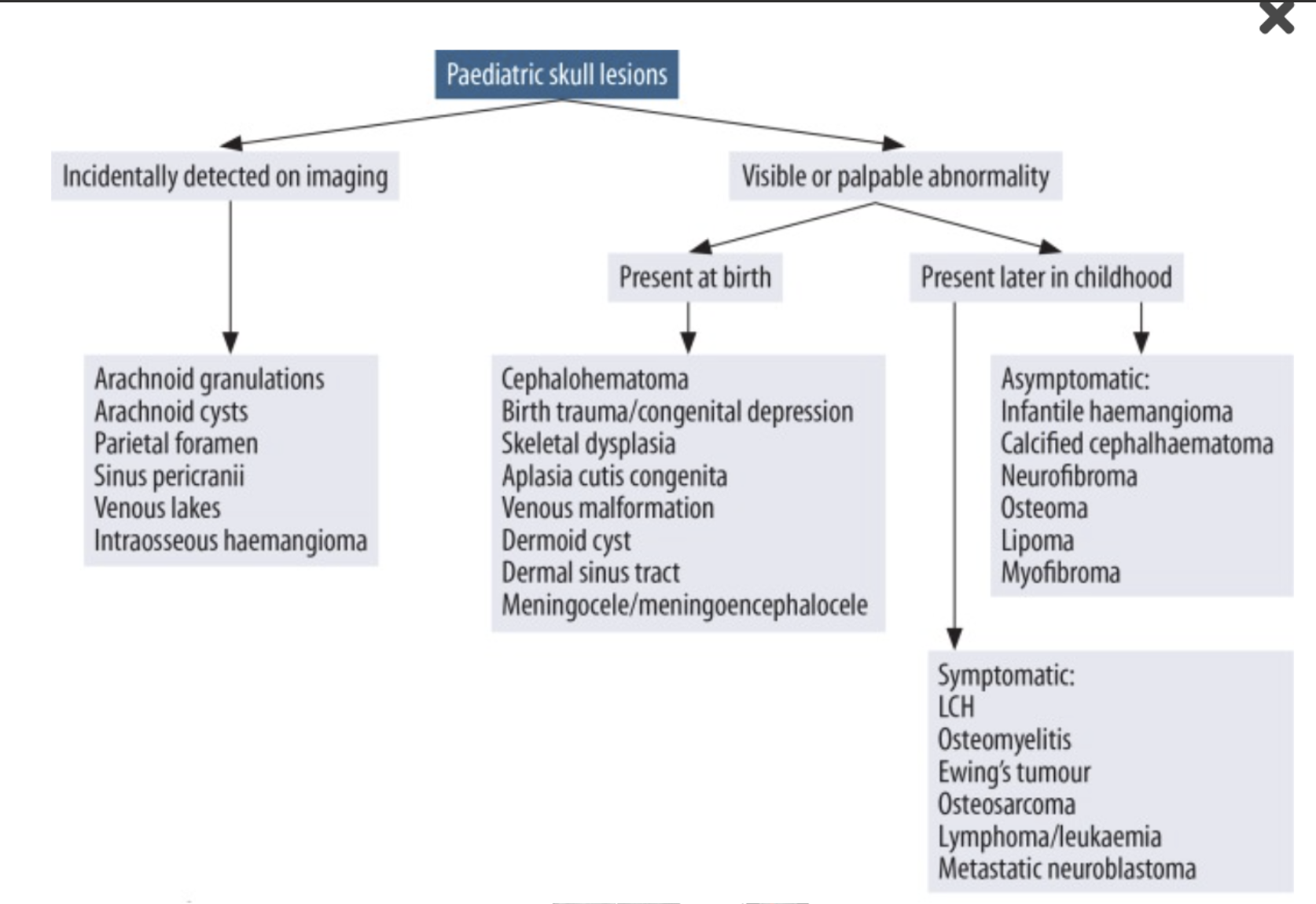
Differential diagnosis
After getting the pocus, outpatient MRI of the orbits with IV contrast and biopsy was scheduled. The diagnosis of Langerhans cell histiocytosis (LCH) was confirmed within 2 weeks. Pt had surgical resection, not requiring any chemotherapy due to early recognition and management.
Langerhan's Cell Histiocytosis
Occurs in kids < 15 years old. It has both neoplastic and inflammatory processes.
Abnormal growth of antigen presenting cells. Can be localized to skin or bony lesion who present disseminated and includes the bone marrow, lungs, liver, spleen, lymph nodes, gastrointestinal tract, and pituitary gland.
Rare but fatal presenting symptoms: Rash that is characterized as scaly papules, nodules, or plaques and can resemble seborrheic dermatitis. Often misdiagnosed as atopic dermatitis (eczema).
Treatment
Range from observation to systemic steroids
Surgical resection
Chemotherapy /radiation
Tama's tips
Bony involvement in the skull occurs in 78% of patients with LCH
Can get plain film imaging to help further characterize "punched out" lesions
Periorbital ecchymosis "racoon eyes"= Metastatic neuroblastoma
References: