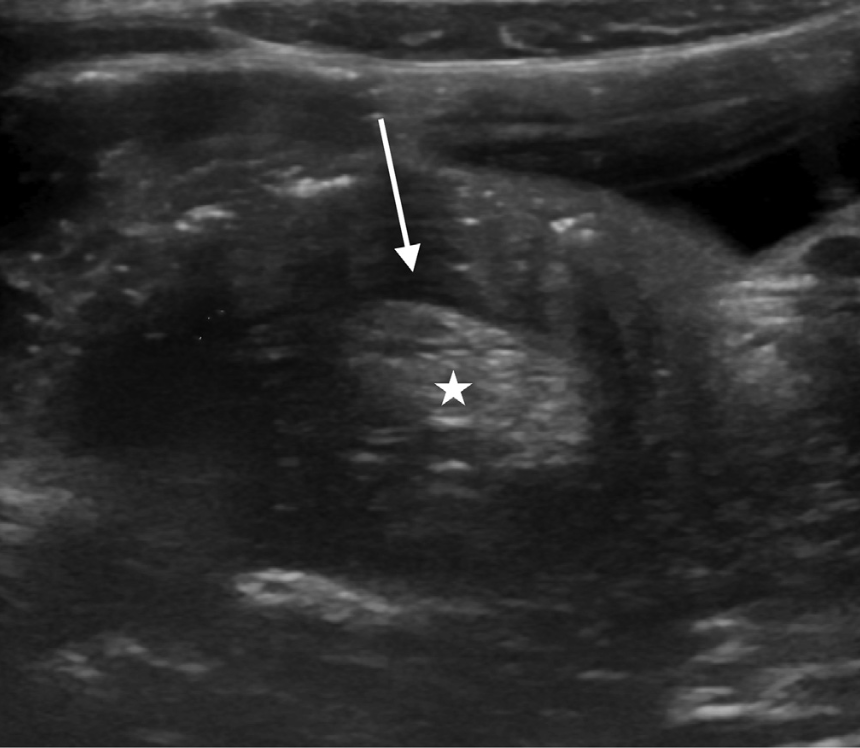
There is mesenteric fat dragged into the intussusception mimics the fatty renal hilum (star), and the hypoechogenic edematous bowel wall resembles the renal parenchyma (arrow). Normal kidney on the top right of the image.
Who should I suspect this disease in?
The incidence of intussusception ranges from 0.24 to 2.4 per 1,000 live births, with boys being affected 2 to 8 times more than girls. Most common among 3-12 months (but in truth can occur at any age, even elderly patients)
How does it present?
The classic triad: colicky abdominal pain, vomiting, and red currant jelly stools occurs in only 21% of cases. Currant jelly stools are observed in only 50% of cases.
Should I do a CT scan on the child?
Ultrasound is the modality of choice and nears 100% sensitivity and specificity. CT is indicated when the ultrasound findings are inconclusive.
What is the treatment?
Stable patients are treated with hydrostatic or pneumatic enema under fluoroscopy or ultrasound. Laparoscopy is indicated for unstable patients or if nonoperative reduction is unsuccessful.
When should I consider it?
A child vomiting without diarrhea should raise suspicion. In addition, consider it in infant/toddler with a change in mental status.
Josh Greenstein, MD FACEP